How lung cancer develops symptoms and signs. Lung cancer - symptoms, signs, causes, diagnosis and treatment. Types of lung cancer by histological principle
Among oncological diseases, lung cancer is considered one of the most common, it is caused by a mutation of the cells that make up the lung tissue. They replace normal cells but cannot function properly.
Unfortunately, the disease is characterized by increased mortality; more than others, men over 50 who abuse tobacco products are more susceptible to it. Over time the group
the risk began to “replenish”, people younger than the specified age, as well as women, are increasingly sick.
Emphasis is placed on a new approach to patient selection using prognostic and predictive factors. The current reality is based on the development of pneumo-oncology centers that can support the ever-increasing demand and complexity of care for bronchogenic carcinoma in our country.
Lung carcinoma is the most common cause of death among malignant tumors worldwide. Although this primacy has existed for many years, one can perceive increasingly optimistic changes in the dissemination of information about the causes of origin, pathogenesis and individual susceptibility to this disease, which leads to the expected extension of the life of patients. By recognizing early morphological changes and, above all, by identifying individual molecules of cellular signaling pathways of carcinogenesis, they aim to develop new technologies for more successful diagnosis and search for new targets for selective treatment.
Statistics on this ailment remains controversial: doctors are still researching it, trying to establish the exact causes of its occurrence, and looking for effective treatments.
It is known for certain that various substances with carcinogenic properties can cause the disease. Experts from the World Health Organization recognize that cigarette smoking carries the greatest risk for the disease. In Russia every year more than sixty thousand people are diagnosed with this disease.
In therapy, fundamental changes are taking place in the development of new drugs, as well as in the choice of patients for whom this treatment is intended. The ratio between men and women is about 3: in men, lung cancer shows the highest morbidity and mortality from all malignant neoplasms. Male mortality declines very little when it declines by about 15% in 25 years.
Stages of lung cancer
The Czech Republic approaches the trend of the most advanced countries in this respect. It is a tumor with a typical tobacco smoke association, and smokers are the most common tumor. Its rise among women is no doubt an unfortunate consequence of the emancipation associated with the increase in women's smoking habits in all developed countries. It is reported that men are associated with smoking up to 90% of cases, women account for about 75%. However, lung cancer is common, in which the seventh is the most common malignancy.
The first or primary, as they are usually called in medical practice, symptoms - coughing with the release of blood, fatigue, the patient begins to lose weight, he develops halitosis. As a rule, with such manifestations, people go to the doctors for help.
Symptoms may be:
- Local, they appear early as a result of blockage of the bronchial lumen by a malignant formation. These include coughing, coughing up blood, shortness of breath and severe pain;
- Secondary, they appear due to the appearance of inflammatory processes, or metastases to other internal organs. Such symptoms are characteristic of advanced stages of cancer;
- In general, they follow tumor intoxication. This is a weakening of the body, fatigue, the patient may also suffer from anorexia, and begins to lose weight. They are called common due to the fact that they themselves are not a direct sign of the disease, manifesting themselves as early stage, and later.
 Let's take a closer look at the symptoms that accompany initial stage diseases:
Let's take a closer look at the symptoms that accompany initial stage diseases:
Treatment of lung cancer folk remedies
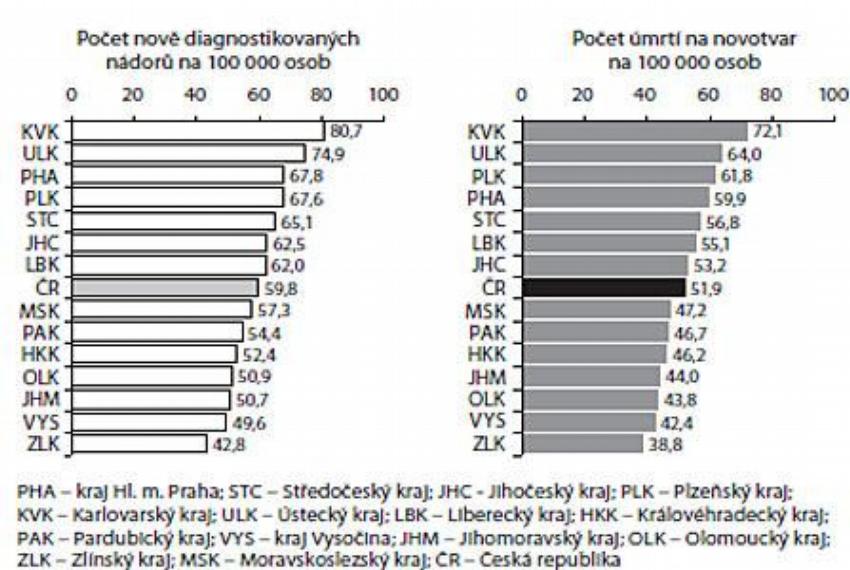
There are relatively large regional differences in our republic. The highest incidence is recorded in the Plzeň and Ústie regions, while the lowest incidence is in the Zlín and Moravian-Silesian regions. The survival rate for lung cancer is shorter than most other solid tumors.
There is no real early detection of lung carcinoma. More than 80% of patients are diagnosed at the time of diagnosis, and there is still a high percentage of patients who are not treated at all. There is a paradoxical situation in trying to improve the diagnosis of early stages. Due to new technologies, it is possible to diagnose pre-invasive lesions, but the availability of this method is not comprehensive, and the treatment of non-invasive mucosal lesions remains questionable. Other diagnostic methods may be used to indicate the stage of staging, but this usually means more frequent demonstration of distant or regional metastases and progression of the disease to higher stages.
- More than half of the patients develop bleeding from the lungs, streaks of scarlet blood appear in the sputum. Only when stage 4 comes, the discharge turns completely red;
- Pain in the chest area is localized in different ways, its intensity may also vary. Symptoms appear depending on where exactly the tumor appeared, pain in most cases is localized at the site of the malignant formation, but occasionally it can also appear on the opposite side;
- Cough, manifested in 85% of those affected by the disease. This is a natural reflex to obturation of the bronchus, at first the cough is dry and hacking, with time it becomes wet, mucopurulent sputum is released with it;
- The degree of manifestation of shortness of breath directly depends on how strong the manifestations in the bronchi are, such a symptom is the result of squeezing of the vessels that provide blood circulation in the lungs. Appears with a probability of 30-40%.
A typical symptom for respiratory cancer in adults is the regular occurrence of obstructive pneumonia, which quickly comes and goes, in men over 50 years of age - this should be of particular concern.
Thus, the health option is refined, but not increased. However, it is encouraging that the real working capacity in our country is growing. There are a number of reasons, but many questions await explanation. Undoubtedly, there is a long period of time when malignant circulation in the lung tissue is not clinically or laboratory recognizable. At the time of diagnosis, the tumor mass is already too large, and the grade of the tumor usually does not allow a radical surgical solution.
In most countries, primary prevention continues to be the most effective way fighting lung cancer and should be a community priority. Regular studies of heavy smokers, however controversial, provide an opportunity to detect lung cancer in the operational phase and change the company's overall vision for the fight against this disease. From a practical clinical point of view, the basic division into two groups with characteristic biological behavior continues to apply.
Lung cancer can also occur without symptoms, making it difficult to diagnose the disease. Clinical picture appears only after the malignant formation begins to grow into other organs, after which the standard signs of oncological disease appear. The severity of shortness of breath directly depends on the size of the tumor. Pain appears in 30-50% of cases, almost always in the area in which the cancer is located.
Non-small cell lung cancer, which accounts for 80% of cases, shows a slower growth rate than small cell carcinoma. From a histological point of view, this is a heterogeneous group, which, for practical reasons, is mainly devoted to small cell lung carcinoma. The main types are squamous cell carcinoma, adenocarcinoma, and large cell carcinoma. In recent years, there has been an increase in the number of cases of adenocarcinoma due to squamous cell carcinoma. In tumors with glandular structures, it is necessary to distinguish bronchioalveolar carcinoma from adenocarcinoma with a bronchiolalveolar component.
 Small cell carcinoma is another form of the disease that occurs in mediastinal lung cancer. It is characterized by extreme malignancy, and rapid germination of metastases. This form is rarely formed, due to uniform seeding of all tissues in the affected area.
Small cell carcinoma is another form of the disease that occurs in mediastinal lung cancer. It is characterized by extreme malignancy, and rapid germination of metastases. This form is rarely formed, due to uniform seeding of all tissues in the affected area.
The main symptoms and signs of lung cancer in women and men
Options for surgical resection for non-small cell lung cancer tends to be greater than for small cells because metastatic deposits occur later. However, the presence of clinically silent micrometastases is relatively high at all stages. Sensitivity to chemotherapy and radiotherapy is still lower than that of small cell bronchogenic carcinoma, although it increases with newer cytostatics.
Small cell bronchogenic carcinoma accounts for 20% of cases. characteristic feature is fast growth with a tendency to create distant metastases, which significantly limits the possibilities surgical treatment. The disease is usually responsive to chemotherapy and radiotherapy, but the response time to treatment is relatively short and relapse treatment is poorly performed. Localized disease is generally considered to be limited to one side of the chest and possibly the same supraclavicular nodes.
The main symptoms are shortness of breath due to damage to a large part of the lung parenchyma. Symptoms appear less often in women, since there are much fewer smokers among them, however, in reality modern life both sexes are increasingly drawn to cigarettes on an equal footing.
Signs of lung cancer
It is necessary to know how cancer manifests itself, because by detecting a sign of the disease in time, you can slow down its development, prevent the disease from going through all 4 stages. The first signs may resemble a common cold, and therefore do not cause concern in patients.
In practice, sometimes a limited disease is considered as such a range of tumors that can be included in the irradiated field. The range of tumor overlapping limited disease is classified as extensive disease, unfortunately common in prevalence. lung tumor may contain a component of small cell carcinoma and, at the same time, cells of a different histological type. Such a tumor is called a combined carcinoma, and treatment is guided by the more malignant variant.
Early signs of lung cancer
For lung cancer, overall survival is estimated to be only 6 months over the last 30 years. However, in some subgroups of patients, we are seeing therapeutic advances that were not possible during the first cytotoxic drugs used for centuries. Undoubtedly, the quality of life of treated patients has improved, improved the tolerance of chemotherapy, greatly improved the tolerance of biological therapy and a number of effective palliative treatments.
These include:
- Periodic cough;
- Fatigue;
- Appetite problems;
- Weight loss.
These manifestations are early, however, if you do not pay attention to them (which is most often the case in men), the malignant formation continues to expand, it gives metastases that penetrate into the internal organs or tissues, after which the pain syndrome begins. None of these signs can be called decisive, since there are no nerve endings in the lungs themselves, pain does not indicate the germination of metastases.
A combination of standard treatments. The current trend is undoubtedly towards more rational combinations of classical treatments such as surgical resection, chemotherapy, radiation therapy and endobronchial therapy. Surgical resection without further treatment of non-small cell carcinoma is only considered in the very early stages.
How the disease progresses
Chemotherapy is used in a number of modifications. He starts talking about the violation of the platinum effectiveness of classical chemotherapy. For small cell lung cancer, chemotherapy is the standard at all stages. Radiation therapy itself may be an alternative to surgical resection for inoperable patients with peripheral tumors or patients who refuse treatment. New treatment systems provide more and more options for curative treatment.
 The tumor grows long enough, and may go unnoticed for several years. There are three main stages of development:
The tumor grows long enough, and may go unnoticed for several years. There are three main stages of development:
- Biological, this is the period that passes from the appearance of a tumor to its detection with an x-ray;
- Asymptomatic, in which the disease can be detected using x-rays, in the absence of symptoms;
- Clinical, in which lung cancer can be detected by signs typical of this disease.
The first two stages are not associated with a significant deterioration in health, however, this is precisely what leads to the fact that the patient does not seek medical help in time. In addition, signs may disguise themselves as other ailments in the second or third stage.
Stereotactic radiation therapy makes it possible to deliver a tumor dose with higher spatial accuracy and minimal damage to healthy tissues. This can be achieved by precise blocking of the body during planning, modeling and treatment. The number of symptomatic ulcerative pneumonitis decreased by less than 5%, but care must be taken near the chest wall, large vessels, esophagus, or spinal cord. More risky patients after pneumonectomy. With radiation therapy respiratory tract the patient is irradiated only at a certain stage of the respiratory cycle.
An unsystematic cough is often mistaken for bronchitis, pneumonia, and other similar pathologies. The temperature "jumps" from high to normal. Such manifestations can be eliminated by medication, but they appear regularly, and it is impossible to leave a suspicious frequency of diseases unattended.
In the presence of symptoms such as shortness of breath, impaired heart rate, pain in the chest, we can talk about the development of the disease up to stage 2-3. This is a direct consequence of the cessation of the work of entire sections of the lungs, after which the quality of life of the patient begins to decline rapidly.
Hyperfractionated radiation therapy did not bring the expected effect. The method can be combined with external beam therapy or used alone or in combination with another endobronchial method. Endobronchial treatment has seen the proliferation of new therapeutic systems that are more effective but increasingly demanding. Laser therapy, electrocoagulation, argon beam, or stent insertion are used, while endobronchial photodynamic therapy has not been performed.
In most cases, endobronchial therapy is used as a palliative procedure to release or simulate large airways. It is associated with symptoms such as shortness of breath, hemoptysis and cough or inflammatory inflammation. Endobronchial therapy can be radical for tumors of a small area on the bronchial mucosa, especially if they are stored in the central airways. Palliative care includes a range of active procedures aimed at reducing the subjective problems caused by the tumor, thereby improving the quality of life of patients.
In the later stages, there are also signs such as a complicated passage of food through the esophagus, which is often confused with its inflammation. Such a manifestation is a consequence of the penetration of metastases into the lymph nodes, which complicate the movement of food.
Signs of pulmonary oncology in women and men are practically the same, the difference is only in the likelihood of occurrence, because it is men who are more prone to smoking.
For lung cancer, this basically means treating shortness of breath, pain, cough, and fever according to various reasons. Specific situations include superior vena cava syndrome, pleural syndrome, and large airway obstruction. Radiation therapy, endobronchial treatment, different types pleurodesitis and, of course, pharmacotherapy, the effectiveness of which has also improved significantly.
Initiation of biologically targeted treatment. As with other malignant neoplasms, biologically targeted therapy is actively used in the treatment of bronchogenic carcinoma. Proactively administered small molecule inhibitors of the epidermal growth factor receptor tyrosine kinase or monoclonal antibodies against these receptors are clearly successful new drugs. Another real group are substances that block the activity of vascular endothelial growth factor. So far, no other more successful treatment structure has been found, although research is underway. wide range tumor vaccines.
Lung Cancer Treatment
Even modern medicine does not give a sure answer whether cancer can be cured. Oncological diseases are still considered incurable, at least in the later stages. In addition, the pulmonary form of oncology is characterized by high mortality, this figure is much higher than that of other varieties.
 Only 16% of patients who managed to live more than five years after the discovery of the disease can answer the question “is lung cancer treated” in the affirmative, but if nothing is done, it becomes almost impossible to live more than four months. However, the presented figures are very arbitrary, since the course of the disease depends on many factors.
Only 16% of patients who managed to live more than five years after the discovery of the disease can answer the question “is lung cancer treated” in the affirmative, but if nothing is done, it becomes almost impossible to live more than four months. However, the presented figures are very arbitrary, since the course of the disease depends on many factors.
Only a thorough analysis of the tumor can determine whether lung cancer is curable, taking into account such factors:
- Type. Small cell oncology manifests itself already at a late stage of development, it progresses very quickly and actively metastasizes;
- The size. The factor is considered formal, it can be used to determine at what stage of development a malignant tumor is;
- Metastases. The subsequent treatment is determined by the rate and nature of their growth, if they are distant, or formed on secondary tumors, treatment through resection may be ineffective.
How to cure cancer:
- Surgical intervention. Traditional treatment involves the removal of the tumor, as well as tissues that are in close proximity. Such a technique is permissible only if metastases have not gone, and the tumor has not occupied a significant part of the lung, otherwise there will be no effect from the operation;
- Chemotherapy. It also refers to the usual measures used to treat lung cancer, which involves the introduction of potent drugs that destroy cancer cells. It works well on the small cell form of the disease, but is associated with significant harm to the body;
- Radiation therapy. It is used as an auxiliary method, it is considered more effective than chemical therapy, but does not give the same effect as surgery;
- Cyber knife. A new word in oncology, used in developed countries. This method is based on the destruction of cancer cells under the influence of X-rays.
 Diagnostics allows you to determine exactly where the cancer is located, a special program creates an irradiation scheme, after which the X-ray machine fires point beams of rays, destroying cancer cells. Of course, this does not give a definitive answer to the question: “how to cure cancer”, using only a cyber-knife you cannot get rid of the disease, however, in combination with other methods, it allows you to achieve significant results.
Diagnostics allows you to determine exactly where the cancer is located, a special program creates an irradiation scheme, after which the X-ray machine fires point beams of rays, destroying cancer cells. Of course, this does not give a definitive answer to the question: “how to cure cancer”, using only a cyber-knife you cannot get rid of the disease, however, in combination with other methods, it allows you to achieve significant results.
Treatment folk remedies It is also often used to treat cancer; for this purpose, various herbs and mushrooms are used. Doctors do not prohibit their use, but like other methods, treatment with soda, herbal infusions and other "improvised" means cannot be effective on its own, it must be combined with other methods.
Diagnosis of lung cancer
Diagnosis is an important part of treatment, early screening allows for the detection of pathology and increases the likelihood of its cure. You need to be attentive to the possible manifestations of the disease, and undergo an examination in time, especially for smokers. The main tool for detecting cancerous tumors is radiography. chest.
 X-rays are taken from the back and side, the results obtained reveal suspicious areas, but cannot establish the presence of a tumor.
X-rays are taken from the back and side, the results obtained reveal suspicious areas, but cannot establish the presence of a tumor.
When suspicions arise, computed tomography is performed, which already in the early stages does not provide enough information. With this form of examination, a large number of cross-sectional images of the whole body, before starting the scan, a contrast agent is injected into the body through a vein, which makes the results more accurate.
There are also other types of examinations using tomography - low-dose or magnetic resonance, they are used to detect small cancers or to obtain the most accurate information about the location of the tumor.
Prevention of lung cancer
As already mentioned, most cancer patients smoke, so avoiding cigarettes will reduce the likelihood of the disease. Unfortunately, there are cases when the disease appears without smoking, however, this relatively small probability is not worth the risk of poisoning your body with nicotine.
Quitting smoking is extremely difficult, and nicotine gum or patches, as well as other drugs, can help along the way. Cancer can even be caused by inhaling tobacco smoke.
It is necessary to avoid the ingestion of carcinogenic substances such as asbestos, radon, arsenic and others. Their inhalation can provoke oncological disease even in those people who have never smoked.
The risk of disease is reduced if you eat vegetables and fruits, alcohol has the opposite effect. Physical activity keeps the lungs healthy, so regular exercise and light jogging. Especially useful are apples containing flavonoids, quercetins and naringinins. If you understand what causes oncological diseases, you can prevent their occurrence.
Learn about unusual signs of lung cancer
Lungs' cancer - malignant tumor of the lung, usually classified as small cell or non-small cell cancer. Cigarette smoking is a major risk factor for most tumor variants. Symptoms include cough, chest discomfort, and, less commonly, hemoptysis, however, many patients are asymptomatic and some develop metastatic lesions. Diagnosis is suspected by chest x-ray or computed tomography and confirmed by biopsy. Treatment is carried out using surgical, chemotherapeutic and radiation therapy methods. Despite advances in therapy, the prognosis is poor and attention should be focused on early detection and prevention of the disease.
Epidemiology
In the United States, approximately 171,900 new cases of respiratory cancer are diagnosed each year and 157,200 deaths are recorded. The incidence increases in women and is likely to stabilize in men. Black men are at particularly high risk.
Causes of lung cancer
Cigarette smoking, including passive smoking, is the most important cause of lung cancer. The risk depends on the age and intensity of smoking, as well as its duration; the risk decreases after smoking cessation, but probably never returns to baseline. For non-smokers, the most important environmental risk factor is exposure to radon, a degradation product of natural radium and uranium. Occupational hazards associated with exposure to radon (miners of uranium mines); asbestos (from builders and workers who destroy buildings, plumbers, shipbuilders and auto mechanics); quartz (for miners and sandblasters); arsenic (in workers associated with copper smelting, pesticide production and plant protection products); chromium derivatives (at stainless steel plants and pigment factories); nickel (at battery and stainless steel plants); chloromethyl ethers; beryllium and emissions from coke ovens (from steel workers) lead to the development of a small number of cases each year. The risk of malignant neoplasms of the respiratory organs is higher with a combination of two factors - occupational hazards and cigarette smoking than with only one of them. COPD and pulmonary fibrosis may increase the risk of developing the disease; preparations containing beta-carotene may increase the risk of developing the disease in smokers. Polluted air and cigar smoke contain carcinogens, but their role in the development of lung cancer has not been proven.
Symptoms of lung cancer
Approximately 25% of all cases of the disease are asymptomatic and discovered incidentally during chest examination. Symptoms of lung cancer consist of local manifestations of the tumor, regional spread and metastases. Paraneoplastic syndromes and general manifestations may occur at any stage.
Local symptoms include cough and, less commonly, dyspnea due to airway obstruction, post-obstructive atelectasis, and lymphatic dissemination. Fever can occur with the development of post-obstructive pneumonia. Up to half of patients complain of vague or limited chest pain. Hemoptysis is less common, blood loss is minimal, except rare cases when a neoplasm destroys a large artery, causing massive bleeding and death due to asphyxia.
Regional spread can cause pleuritic pain or dyspnoea due to pleural effusion, dysphonia due to tumor invasion into the recurrent laryngeal nerve, dyspnea, and hypoxia due to diaphragmatic paralysis with involvement of the phrenic nerve.
Compression or invasion of the superior vena cava (superior vena cava syndrome) can lead to headache or fullness in the head, swelling of the face or upper extremities, shortness of breath, and redness (plethora) when lying on the back. Manifestations of the syndrome of the superior vena cava - swelling of the face and upper limbs, swelling of the cervical and saphenous veins of the face and upper half of the body and hyperemia of the face and body. Superior vena cava syndrome is more common in patients with a small cell appearance.
Apical masses, usually non-small cell, may invade the brachial plexus, pleura, or ribs, causing shoulder and upper limb pain and weakness or atrophy of one arm (Pancoast tumor). Horner's syndrome (ptosis, miosis, anophthalmos and anhidrosis) develops when the paravertebral sympathetic chain or cervical stellate ganglion is involved in the process. Extension to the pericardium may be asymptomatic or lead to constrictive pericarditis or cardiac tamponade. Rarely, compression of the esophagus leads to dysphagia.
Metastases always, ultimately, cause manifestations associated with their localization. Liver metastases cause gastrointestinal symptoms and eventually liver failure. Metastases to the brain lead to behavioral disturbances, amnesia, aphasia, convulsions, paresis or paralysis, nausea and vomiting, and ultimately coma and death. Bone metastases cause intense pain and pathological fractures. Malignant neoplasms of the respiratory system often metastasize to the adrenal glands, but rarely lead to adrenal insufficiency.
Paraneoplastic syndromes are not directly caused by cancer. Common paraneoplastic syndromes in patients are hypercalcemia (caused by tumor production of a protein associated with parathyroid hormone), syndrome of inappropriate secretion of antidiuretic hormone (SIADH), thickening of the terminal phalanges of the fingers with or without hypertrophic osteoarthropathy, hypercoagulability with migratory superficial thrombophlebitis (Trousseau's syndrome), myasthenia gravis (Eaton-Lambert syndrome) and a variety of neurological syndromes, including neuropathies, encephalopathies, encephalitis, myelopathy, and cerebellar lesions. The mechanism of development of neuromuscular syndromes involves the expression of autoantigens by the tumor with the formation of autoantibodies, but the cause of most others is unknown.
Common symptoms usually include weight loss, malaise, and are sometimes the first manifestations of malignancy.
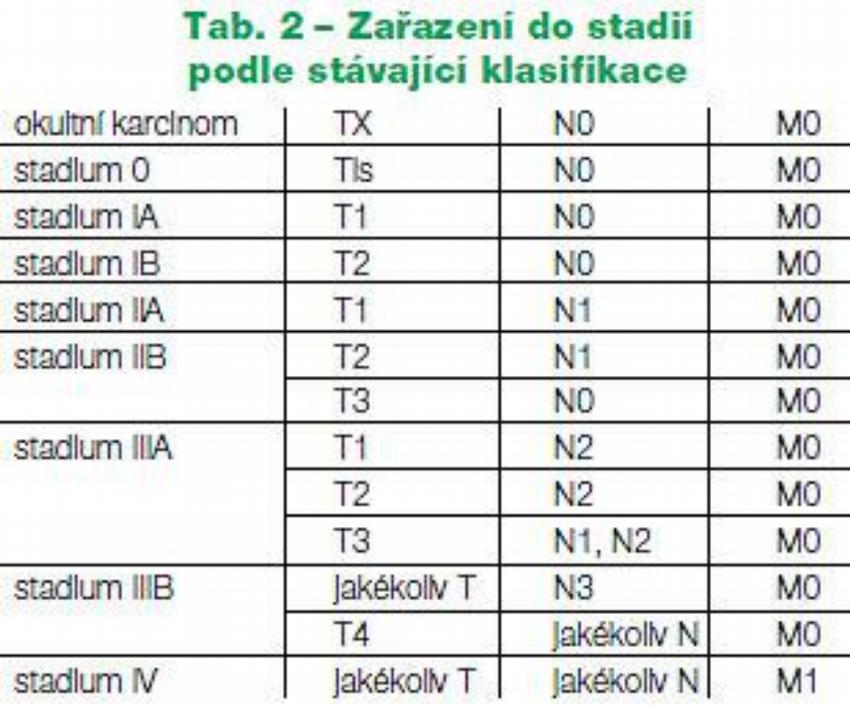
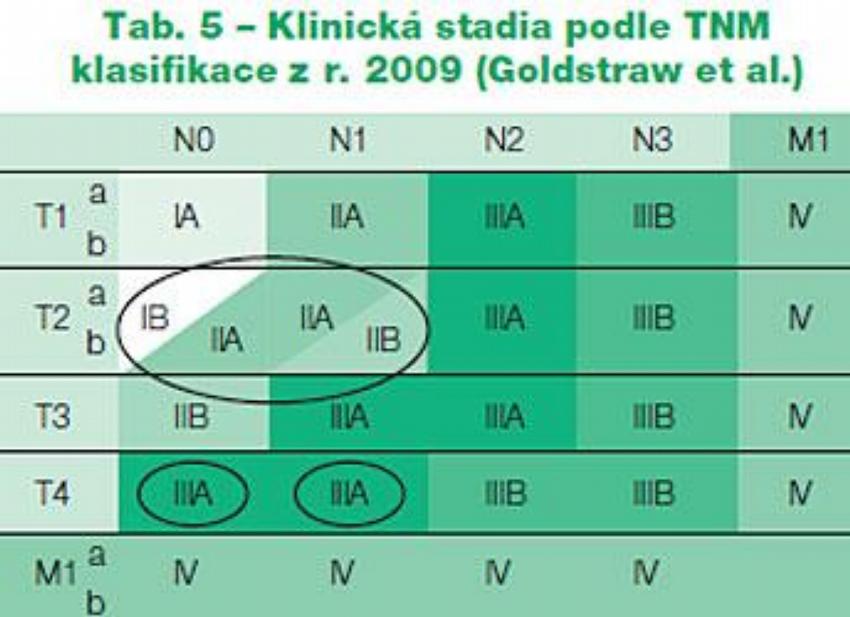
stages
| primary tumor | |
| Tis | Carcinoma in situ |
| T1 | Bronchial tumor (i.e. not in the main bronchus) |
| T2 | Tumor with any of the following: >3cm Involves the main bronchus > 2 cm distal to the carina Invades the visceral pleura Atelectasis or post-obstructive pneumonia that extends to the root but does not involve the entire lung |
| TK | Invades the chest wall (including neoplasms of the superior sulcus), diaphragm, mediastinal pleura, or parietal pericardium Main bronchus involved |
| T4 | A tumor of any size with any of the following features: Grows into the mediastinum, heart, large vessels, trachea, esophagus, vertebral body, carina Malignant pleural or pericardial effusion Satellite nodules of neoplasm within the same lobe as the primary tumor |
| Regional lymph nodes (N) | |
| N0 | No metastases to regional lymph nodes |
| N1 | Unilateral metastases to peribronchial lymph nodes and / or lymph nodes of the root of the lung and intrapulmonary lymph nodes located on the path of direct spread of the primary neoplasm |
| N2 | Unilateral metastases to mediastinal and/or subcarinal lymph nodes |
| N3 | Metastases to contralateral mediastinal nodes, contralateral root nodes, scalene muscle of the corresponding side, or contralateral or supraclavicular lymph nodes |
| Distant metastases (M) | |
| М0 | No distant metastases |
| M1 | Distant metastases are present (including metastatic nodes in the lobes of the relevant side, but distinct from the primary tumor) |
Forms
Malignant
- Carcinoma
- small cell
- Oat cell
- transitional cell
- mixed
- Non-small cell
- Adenocarcinoma
- acinar
- Bronchioalveolar
- papillary
- solid
- Adenosquamous
- Large cell
- clear cell
- giant cell
- Squamous
- Spindle cell
- Carcinoma of the bronchial glands
- Adenoid cystic
- Mucoepidermoid
- Carcinoid
- Lymphoma
- Primary pulmonary Hodgkin's
- Primary pulmonary non-Hodgkin's
benign
- Laryngotracheobronchial
- Adenoma
- Hamartoma
- myoblastoma
- Papilloma
- Parenchymal
- Fibroma
- Hamartoma
- Leiomyoma
- Lipoma
- Neurofibroma/schwannoma
- Sclerosing hemangioma
For malignant cell transformation respiratory epithelium prolonged contact with carcinogenic substances and the accumulation of multiple genetic mutations are required. Mutations in genes that stimulate cell growth (K-RAS, MCC), encode growth factor receptors (EGFR, HER2/neu) and inhibit apoptosis (BCL-2) contribute to the proliferation of pathological cells. Mutations that inhibit tumor suppressor genes (p53, APC) have the same effect. When sufficient accumulation of these mutations occurs, malignant neoplasm respiratory organs.
Lung cancer is usually classified into small cell (SCLC) and non-small cell (NSCLC). Small cell is a very aggressive neoplasm, almost always occurs in smokers and causes widespread metastasis in 60% of patients by the time of diagnosis. The symptoms of the non-small cell species are more variable and depend on the histological type.
Complications and consequences
To treat a malignant pleural effusion, a thoracentesis is first performed. Asymptomatic effusions do not require therapy; symptomatic effusions that recur despite multiple thoracocentesis are drained through a chest tube. Injection of talc (or sometimes tetracycline or bleomycin) into the pleural cavity (a procedure called pleurodesis) hardens the pleura, eliminates the pleural cavity, and is effective in more than 90% of cases.
Treatment for superior vena cava syndrome is similar to lung cancer treatment with chemotherapy, radiation therapy, or both. Glucocorticoids are commonly used, but their effectiveness has not been proven. Apical tumors are treated surgical methods with or without preoperative radiotherapy or radiotherapy with or without adjuvant chemotherapy. Therapy for paraneoplastic syndromes depends on the specific situation.
Diagnosis of lung cancer
The first examination is a chest x-ray. It clearly identifies certain lesions, such as single or multiple infiltrates or an isolated nodule in the lung, or more subtle changes, such as thickened interlobar pleura, mediastinal enlargement, tracheobronchial constriction, atelectasis, non-resolving parenchymal infiltrate, cavitary lesions, or unexplained pleural effusions or effusions. These findings are suspicious, but not diagnostic for lung cancer, and require further investigation using high-resolution CT (HRCT) and cytological confirmation.
A CT scan can reveal many characteristic structures and changes that help confirm the diagnosis. CT-guided needle biopsy of accessible lesions can also be performed and is important in staging.
Methods for cellular or tissue diagnostics depend on the availability of tissue and the location of the lesions. Sputum or pleural fluid analysis - least invasive method. In patients with a productive cough, sputum samples obtained upon awakening may contain high concentrations of malignant cells, but the effectiveness of this method does not exceed 50%. Pleural fluid is another convenient source of cells, but effusion occurs in no more than a third of all cases; however, the presence of a malignant effusion is indicative of at least stage IIIB malignancy and is a poor prognostic sign. In general, false negative results cytological studies can be minimized by collecting as much sputum or fluid as possible early in the day and immediately transporting specimens to the laboratory to reduce processing delays that lead to cell breakdown. Percutaneous biopsy is the next of the less invasive procedures. It is more important in diagnosing metastatic sites (supraclavicular or other peripheral lymph nodes, pleura, liver, and adrenal glands) than for lung lesions due to a 20-25% risk of pneumothorax and the risk of false negative results, which probably will not change the accepted tactics. treatment.
Bronchoscopy is the procedure most commonly used for diagnosis. Theoretically, the method of choice for obtaining tissue is the one that is least invasive. In practice, bronchoscopy is often performed in addition to or instead of less invasive procedures, because diagnostic possibilities are higher and because bronchoscopy is important for staging. Combination of wash water examination, brush biopsy and fine needle biopsy of visible endobronchial lesions and paratracheal, subcarinal, mediastinal and lymph nodes root of the lung allows you to establish a diagnosis in 90-100% of cases.






