ECG with dextrocardia electrodes. Dextrocardia on ecg
Dextrocardia - what is it? Dextrocardia belongs to the category of congenital diseases, characterized by improper placement of the heart muscle. That is, we can conclude that such a pathology is characterized by the right-sided placement of the myocardium, despite the fact that in a healthy person it is located on the left side of the chest. But in fact, two forms of the disease are distinguished - this is true dextrocardia and dextrocardia of the heart. With the true type of the disease, a congenital pathology is observed, moreover, in the second case, the disease can be acquired in nature and pathologies in the chest area often become its cause.
The complicated type of dextrocardia is accompanied by various minor or complex pathologies.
Given the characteristics of different types of the disease, we can conclude that the congenital form cannot be treated, while the acquired disease is not only possible, but must be treated. Very often, the signs of such a disease can be distinguished even at the stage of intrauterine development of the fetus; during an ultrasound scan of the fetus, it can be recognized that the child’s heart develops in the right side of the chest, and not in the left.
Important! Often, the right-sided location of the heart may be accompanied by a shift in the opposite direction and other internal organs, and this is a very serious and dangerous pathology.
To date, it has not been possible to clearly identify the causes or risk factors that can provoke the occurrence of such a disease. But there is an assumption that in most cases such an ailment is hereditary, that is, it can develop against the background of a genetic predisposition.
How the disease manifests itself
Cardiac dextrocardia is very often asymptomatic, especially if it is not accompanied by concomitant diseases. But it is important to note that this disease is characterized by the presence of a period of exacerbation, during this period pain in the chest area may appear. In newborns, this disease can manifest itself with symptoms characteristic of jaundice. That is, children with such a diagnosis can be born with the presence of yellowing in the area of \u200b\u200bthe eyes and skin. In addition, there may be difficulty breathing, passivity and pallor of the skin. Children with such a diagnosis are under increased supervision of specialists, and all because there is a risk of developing sudden death syndrome.
Sometimes infants with dextrocardia have various pathologies of the abdominal and pleural organs.
As for the acquired form of the disease, it is extremely rare, but at the same time it is very dangerous and can be accompanied by very pronounced symptoms, such as an unstable pulse and rapid breathing. If such signs occur, it is important to seek help from specialists as soon as possible, who will conduct all the necessary examinations and prescribe the most optimal treatment.
Attention! At congenital form patients should be under medical supervision at all times. Moreover, a special method of treatment is being developed for them, which they must strictly adhere to.
Dextrocardia: ECG diagnostic method
Since such a pathology is often congenital, it is not surprising that it is diagnosed even at the stage of intrauterine development of the fetus. But be that as it may, after the birth of a child, a complete diagnosis is carried out, which allows you to determine how the rest of the internal organs are located, as well as to identify the features of the disease itself. It is also worth noting that with dextrocardia ECG- required method diagnostics, in order to make sure that there are no other concomitant diseases of the cardiovascular system that may pose a direct threat to the patient's life.
Diagnosis of such a disease can involve both hardware and laboratory examinations; the main hardware methods for diagnosing a disease include:
- X-ray examination of the chest;
- ECG and echocardiography;
- ultrasound examination of organs abdominal cavity.
It is important to understand that only with a comprehensive examination can one get a truly complete picture of the disease, and only under this condition can one understand how to treat the pathology. Sometimes in order to get a complete clinical picture patients may be prescribed magnetic resonance imaging, but it is prescribed as additional method examinations.
As for the treatment of dextrocardia, such a pathology does not need additional treatment, it is enough just to adhere preventive measures, which will eliminate the likelihood of progression of the disease. But there are cases when such a disease is accompanied by heart defects, and in this case, the patient may be shown surgical intervention. If dextrocardia on the ECG manifested itself in childhood without the presence of aggravating circumstances, then, most likely, the patient will be prescribed drug therapy which may include taking the following medications:
- Immunostimulants.
- Diuretics.
- ACE inhibitors.
- inotropic agents.
This conservative treatment therefore, it cannot exclude the need for surgical intervention. It is also worth noting that if the patient is shown surgery, then, most likely, he will have to undergo a course of antibiotic therapy. But antibiotic therapy can only be carried out for a certain period. The fact is that prolonged use of antibiotics can adversely affect the work of systems and organs important for human health.

Manifestations of the disease on the ECG
As for the complications that may arise if the recommendations of specialists in the treatment of pathology are not followed, then disability and even death can be considered the most dangerous consequences. If you strictly follow all the doctor's prescriptions, then patients with such a diagnosis can live long enough without experiencing serious health problems. You can find out how a person with such a diagnosis might look by looking at a photo of dextrocardia.
Preventive measures
As already noted, in order to feel good with such a disease, and to exclude the likelihood of complications, it is necessary to adhere to the preventive methods prescribed by the specialist. The main prevention of complications of such a disease, of course, can be considered supportive therapy, which may consist of taking medications and undergoing useful procedures. In addition, it is important to note that patients diagnosed with dextrocardia should be very careful about physical activity, since active sports and excessive loads are contraindicated for them.
Dextrocardia
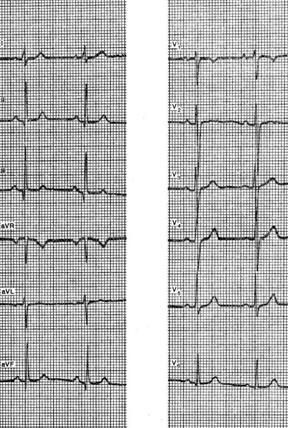
With dextrocardia (situs inversus), all parameters of the electrical position of the heart are mirrored to the right of the midline. The P wave will be inverted in lead I and the QRS axis (âQRS) will be tilted into the right lower quadrant (+90° to +180°). There will be no normal development of the complex from rS to qR to leads V5-V6 in the precordial leads, but it will be observed in leads located symmetrically on the right side of the chest (V3R-V6R) (Fig. 1). More often than dextrocardia, there is a situation in which electrodes incorrectly applied to the upper limbs simulate dextrocardia in the frontal plane, but this is not confirmed in the precordial leads.
Rice. 1. Dextrocardia. Note: mirror electrocardiographic patterns, all vectors are directed to the right. The right precordial leads register LV vectors, which are normally recorded on the left.
Repolarization
At the end of the QRS complex, the ECG returns to the baseline, where it remains for 150-200 ms before the onset of the T wave with its gentle onset and steep return to the baseline. The period between the end of the QRS complex and the beginning of the T wave is called the ST segment, and the connection of the QRS complex and the ST segment is called the J point. The ST segment can be slightly elevated above the isoline (0.5-1 mm) in leads with a high R wave, as well as in right precordial leads (V1-V2) with a dominant S wave. The most common variant of the norm, manifested by ST elevation ≥1 mm in many leads, is called the "early repolarization" syndrome. Often it is due to an increase in the tone of the vagus nerve and can serve as a reason for differential diagnosis with pericarditis or myocardial ischemia (Fig. 2).

Rice. 2. "Early repolarization" syndrome in a healthy 20-year-old man. Note ST-segment elevation in most leads, stable over time, without any symptoms of heart disease. Note also the high QRS voltage in the inferior and precordial leads, which could indicate LV enlargement, but this is normal for a 20 year old. The blue arrow points to a normal low-amplitude U wave.
The T wave is normally positive in leads I, II, aVL, and V2-V6, but may be different in other leads. The mean axis of the T wave (âT) in the leads in the frontal plane is ‹60° with respect to the âQRS. The T wave may be negative in the right precordial leads (V1-V3) in children until there is no loss of RV physiological dominance, and is also normal in Black African women and men.
The T wave is followed by a low-amplitude, rounded U wave, which is most commonly seen in the precordial leads (see Figure 2). The U wave reflects delayed repolarization of slow response myocardium and possibly Purkinje fibers.
Francisco G. Cosío, José Palacios, Agustin Pastor, Ambrosio Núñez
Electrocardiography
Dextrocardia is called a congenital pathology, which is characterized by a displacement of the heart to the right side. In this case, all vessels are also mirrored with respect to their normal placement. This defect is quite rare - only 0.01% of the total population.
Many people live with dextrocardia all their lives without experiencing any discomfort. But very often this pathology is combined with other malformations of the heart. Therefore, it must be identified in a timely manner in order to take all measures to preserve the normal life of a person.
Varieties of dextrocardia
Dextrocardia in the fetus can proceed in different ways. Based on the severity of the condition, the following types are distinguished:
- simple. Characterized by atypical placement of the heart (right). At the same time, there are no concomitant pathologies, and the person leads a normal life;
- dextrocardia, which is accompanied not only by a displacement of the heart, but also by other organs. This pathological process usually involves the digestive and respiratory systems;
- complicated. In this case, the heart is located on the right and there are other dangerous malformations of its development.
Also, dextrocardia can be isolated or complete. In the first case, only the heart changes its normal position, and in the second, all the organs of the chest and abdominal cavity. Allocate and partially combined dextrocardia. It is characterized by displacements of organs that are located in the chest.
Primary or secondary dextrocardia
True or primary consider dextrocardia, which was formed as a result of congenital malformations of the fetus. If this pathology arose later, it is called secondary. It is formed against the background of some negative processes in the body:
- with pulmonary atelectasis. Formed when an air blockage occurs;
- with pneumothorax. Manifested by the accumulation of air masses in the pleural cavity. It develops in the presence of certain diseases or after injuries;
- with hydrothorax. It is characterized by the accumulation of fluid in the pleural region due to certain diseases of the heart, kidneys, etc.;
- the presence of a tumor that reaches a huge size.
Reasons for the development of dextrocardia
The heart tube during the development of the fetus is laid in the early stages of pregnancy (up to 10 weeks). It is its deformation that leads to the displacement of organs to the right side. Most often, this pathological condition develops due to gene mutation. Therefore, dextrocardia is considered an autosomal recessive disease that is transmitted from parents to children in the presence of certain favorable factors.

Despite a clear track hereditary causes the formation of pathology, the exact mechanism of its development is unknown. Many people with this disorder do not have serious health problems and their hearts work normally. Children born with dextrocardia are at risk and are constantly monitored by doctors for the timely detection of other abnormalities.
Why is dextrocardia dangerous?
By itself, dextrocardia does not pose a serious danger to human life. The main problems arise only when it is necessary to carry out various diagnostic procedures or surgical intervention, where the risk of medical errors increases several times. They can occur if this pathology has not been previously identified or when the medical worker is not qualified enough.
Also, in the presence of dextrocardia in a person, other comorbidities are very often found:
- . Several defects are detected at once - narrowing of the exit and hypertrophy of the right ventricle, ventricular septal defect, aortic dextraposition;
- other extremely dangerous heart defects that lead to;
- heterotaxic syndrome. Manifested by the absence or insufficient functioning of the spleen;
- primary ciliary dyskinesia. With this disease, the motor function of the cilia of the respiratory tract is disturbed. As a result of this problem, a person often has more bronchitis, sinusitis, otitis media. In men, infertility is observed;
- trisomy. It is a disease that develops against the background of chromosome mutation. It is characterized by the presence of multiple malformations, structural and work defects. nervous system, external deformities (splitting upper lip, changes in the genital organs, etc.). With the development of this anomaly, the child usually dies in utero. At birth, life expectancy does not exceed 5 years.

What symptoms indicate dextrocardia?
Simple dextrocardia, which is not combined with other malformations, is asymptomatic. It cannot be determined without additional diagnostic procedures. But if this problem is combined with other pathologies of the heart and lungs, the following symptoms appear in early childhood:
- pallor of the skin, which can turn into. This sign becomes especially obvious when the child cries;
- there is marked weakness;
- development of shortness of breath;
- in a newborn, yellowness of the sclera of the eyes and skin persists for a long time;
- is revealed;
- delay in physical development;
- frequent respiratory infections.

Diagnosis of dextrocardia
The very first diagnostic procedure for a newborn is an examination by a neonatologist, which is performed on the first day of life. He listens to the chest at typical points, which allows you to identify possible deviations.
If any violations are detected, additional diagnostic procedures are prescribed:
- ultrasound. Ultrasound examination of the heart can be performed even in the maternity hospital. With the help of this procedure, the position of the heart and blood vessels, their structure is determined. Ultrasound is completely safe for young children;
- . An electrocardiogram for young children is performed using sedatives. Even a slight movement during the procedure leads to a distortion of the results. The obtained ECG indicators with dextrocardia seem to change places. At first glance, it seems that the doctor installed the electrodes incorrectly. ECG is of great diagnostic value, since it can be used to differentiate dextrocardia from other pathologies of the heart;
- x-ray diagnostics;

Treatment of dextrocardia
In the presence of simple dextrocardia, treatment is not prescribed. Such people only need to undergo preventive examinations from time to time to identify other possible deviations.
If additional heart defects are identified, doctors resort to surgical intervention. This is necessary to ensure the normal process of blood circulation, which otherwise will lead to death. Also, such children in the preoperative and postoperative period prescribed certain drugs.
These are diuretics, cardiac glycosides and ACE blockers. They allow you to maintain the normal functioning of the myocardium, which is very important at the stage of recovery after surgery and in preparation for it. Antibiotics are also prescribed after surgery to prevent infections.
Many people are interested in what dextrocardia is. This term is understood as a rather rare congenital defect, which is accompanied by a deviation of the heart and large vessels to the right side. This happens symmetrically towards the middle of the body. Pathology is quite rare - according to statistics, its frequency is approximately 0.01%. However, it has practically no clinical manifestations.
The development of the heart tube in the fetus begins in the first trimester of pregnancy. When it is bent to the right, a shift is observed. As a consequence, the heart and great vessels may form on the right side. ICD-10 code for this pathology: Q24.0 Dextrocardia.
In addition to this anomaly, other diseases caused by genetic changes can occur in the fetus. The most frequently mutated genes are Pitxz, ZIC3Shh, HAND, ACVR2. Scientists suggest that the anomaly can be inherited. However, the exact causes of the development of pathology have not been established.
In most cases, the heart functions normally when dextrocardia is present. The child grows and develops without facing the symptoms of the defect. However, such patients should remain under the supervision of a physician, as they are at risk for developing heart disease.
Kinds
The classification of pathology includes the following varieties:
- Unisolated dextrocardia. In this case, all internal organs are located transpositionally. This means that they are mirrored in relation to the normal state.
- Isolated dextrocardia. With this form of the disease, unpaired organs, such as the spleen, liver, stomach, have a normal location. Taking into account the state of the heart chambers, this type of disease is divided into 2 categories - with and without inversion of the atria and ventricles.
 Dextrocardia of the heart is often supplemented by other pathologies:
Dextrocardia of the heart is often supplemented by other pathologies:

Symptoms
Dextrocardia is a manifestation of an abnormal structure of the heart. With a simple form of this condition, which is not characterized by congenital abnormalities, there are no symptoms. Pathological localization of the heart is usually detected in childhood. Sometimes it is also diagnosed in an adult who went to the doctor with another disease.
With such a diagnosis, people do not experience a violation of the condition and there is a completely normal state of health. However, they are prone to respiratory pathologies.
If other organs are affected, there is a risk of such signs:

If dextrocardia develops in the fetus, indicated symptoms found in a newborn. The baby has respiratory problems, signs of jaundice, blanching of the dermis, general weakness.
If a mirror arrangement of the heart is found, the severity of the manifestations will depend on the severity of the damage to the internal organs.
IT IS IMPORTANT TO KNOW! No more shortness of breath, headaches, pressure surges and other symptoms of HYPERTENSION! Find out the method our readers use to treat pressure... Learn the method...
Complications
In the absence of concomitant diseases, dextrocardia does not pose any health hazard and does not affect life expectancy. However, the unusual location of nearby organs can make it difficult to diagnose other diseases and provoke such consequences as:

Diagnosis of dextrocardia
With a congenital form of pathology, it can be detected immediately after the birth of the child. The key task of diagnostics is to identify the localization of other organs and identify abnormal processes in them. In addition, other pathologies of the heart and blood vessels should be excluded.
The key diagnostic method is electrocardiography (ECG). For infants, the procedure is carried out after the use of sedatives. Otherwise, there is a risk of disrupting the recording of the electrocardiogram and obtaining incorrect information.
If an ECG is performed with dextrocardia with the usual application of electrodes, with a mirror arrangement of the heart, teeth of the opposite direction can be detected. It should be borne in mind that dextrocardia on the ECG has important feature: it is characterized by a sharp drop in voltage. 
It is necessary to take an ECG for the diagnosis of other cardiac pathologies by applying a yellow electrode to right hand. In this case, red - should be placed on the left hand.
The examination scheme necessarily includes ultrasound and x-rays. The first procedure is performed to examine the abdominal organs.
Radiography makes it possible to identify the pathological location of the heart. If a person has dextrocardia, an x-ray and description will give a clear picture of the heart and its contours. Such a snapshot helps to detect all changes.
In addition, the following studies can be carried out:

Important: The most significant diagnostic method is electrocardiography. It is this procedure that allows you to confirm or refute the diagnosis. It also allows you to choose methods for differential diagnosis.
Treatment
In most cases, dextrocardia is asymptomatic, so treatment is not carried out. If the baby has heart problems, it may be necessary to perform an operation. If necessary, before surgery, the child is prescribed drugs that increase the intensity of the heartbeat and reduce pressure.
If a person has Kartagener's syndrome, he is prescribed symptomatic remedies:
- expectorants and preparations for cleansing mucus;
- diuretics;
- antihypertensive drugs to reduce pressure;
- antibiotics to eliminate bacterial complications.
 Typically, people with this diagnosis do not experience a decrease in life expectancy. With an isolated form of anomaly, congenital malformations are much more common, which increases the likelihood dangerous consequences for health.
Typically, people with this diagnosis do not experience a decrease in life expectancy. With an isolated form of anomaly, congenital malformations are much more common, which increases the likelihood dangerous consequences for health.
Many people are interested in whether they take the army with such a diagnosis. During the normal functioning of the internal organs, this condition is not a basis for exemption from military service. In the presence of abnormal changes, the decision on the suitability of the conscript is made by a special commission.
Prevention
Since the disease is congenital in nature, it can be very problematic to find effective prevention. At the stage of pregnancy planning, you should consult with a geneticist. This will help select adequate therapy to prevent dextrocardia in the fetus.
Sick children are prescribed medications and supportive care for preventive purposes. This will help prevent the progression of the disease. Usually such people are forced to take all their lives medicines and dose physical activity.
Dextrocardia is a pathology that only in certain cases can lead to various complications. But to avoid negative consequences for health, it is necessary to consult a doctor in a timely manner and strictly follow his recommendations.
Do you have any questions? Ask them in the comments!
ECG practically healthy people with the reverse arrangement of the internal organs (situs viscerum inversus) is characterized by a change in the direction of the main teeth in most leads compared to their direction in the norm. This is due to a change in the location of the heart and its departments: the heart is located in the chest on the right, and its right and left halves change places (180 ° rotation around the longitudinal axis). The mean vectors P, QRS and T are oriented to the right and down, respectively.
As a result, on ECG in lead I, negative P and T waves are recorded and the main wave of the QRS complex is directed downward from the isoline (S or Q wave). Small initial and final teeth of the QRS complex are written down as teeth r1, r. Due to this orientation of the mean vectors of QRS and T, the teeth of RIII and TIII become higher, respectively, of the teeth of RII and TII. PII wave is usually negative or flattened PIII is positive. The shape and direction of the waveforms in leads aVL and aVR change (the waveforms in lead aVR are similar to the waveforms in lead aVL in a normal ECG and vice versa). In lead aVF, only the P wave changes. In the chest leads from V1 to V6, the S wave predominates in the QRS complex or Q is pronounced.
In addition, there is a decrease voltage all teeth from lead to lead from right to left (from V3 to V6). The P wave in the right chest leads is positive, in the left it is negative. According to these signs, in generally accepted leads, a conclusion is made about dextrocardia.
To detect myocardial changes with dextrocardia, the following technique is used: the red electrode is moved from the right hand to the left, and the yellow electrode is applied to the right hand. At the same time, in healthy people, normal teeth are recorded in the limb leads. The chest leads are removed from the left and right halves of the chest in the following order: V2, V1, V3R - V6R. In these leads, the direction of the teeth and the increase in their amplitude correspond to the normal relationship of the teeth in leads V1 - V6 with the usual location of the heart.
At dextroversion(or dextroposition) on the ECG (ECG of a woman K., 53 years old), as well as with dextrocardia, the R wave is reduced in I, aVL and in the left chest leads and RV1, V2 is increased.
The essential difference dextroversion from dextrocardia is a positive P wave in all standard and left chest leads. The latter is due to the usual location of the heart in relation to its longitudinal axis: the right atrium and ventricle on the right, the left on the left. As a result, the atria are excited from right to left (to "+" I and V6 leads) and down (to + I, III leads), the interventricular septum - from left to right (to "-" I, II, aVL, V4 - V6 leads and to " + "Vp V2), left ventricle - to the left (to "+" I, II, aVL, V4-V6 leads).
The latter leads to the form QRI,II,aVL,V4-V6 with relatively low R waves due to the location of the heart on the right.

Many people are interested in what dextrocardia is. This term is understood as a rather rare congenital defect, which is accompanied by a deviation of the heart and large vessels to the right side. This happens symmetrically towards the middle of the body. Pathology is quite rare - according to statistics, its frequency is approximately 0.01%. However, it has practically no clinical manifestations.
The development of the heart tube in the fetus begins in the first trimester of pregnancy. When it is bent to the right, a shift is observed. As a consequence, the heart and great vessels may form on the right side. ICD-10 code for this pathology: Q24.0 Dextrocardia.
In addition to this anomaly, other diseases caused by genetic changes can occur in the fetus. The most frequently mutated genes are Pitxz, ZIC3Shh, HAND, ACVR2. Scientists suggest that the anomaly can be inherited. However, the exact causes of the development of pathology have not been established.
In most cases, the heart functions normally when dextrocardia is present. The child grows and develops without facing the symptoms of the defect. However, such patients should remain under the supervision of a physician, as they are at risk for developing heart disease.
Kinds
The classification of pathology includes the following varieties:
- Unisolated dextrocardia. In this case, all internal organs are located transpositionally. This means that they are mirrored in relation to the normal state.
- Isolated dextrocardia. With this form of the disease, unpaired organs, such as the spleen, liver, stomach, have a normal location. Taking into account the state of the heart chambers, this type of disease is divided into 2 categories - with and without inversion of the atria and ventricles.
 Dextrocardia of the heart is often supplemented by other pathologies:
Dextrocardia of the heart is often supplemented by other pathologies:
Symptoms
Dextrocardia is a manifestation of an abnormal structure of the heart. With a simple form of this condition, which is not characterized by congenital abnormalities, there are no symptoms. Pathological localization of the heart is usually detected in childhood. Sometimes it is also diagnosed in an adult who went to the doctor with another disease.
With such a diagnosis, people do not experience a violation of the condition and there is a completely normal state of health. However, they are prone to respiratory pathologies.
If other organs are affected, there is a risk of such signs:
If dextrocardia develops in the fetus, these symptoms are detected in a newborn child. The baby has respiratory problems, signs of jaundice, blanching of the dermis, general weakness.
If a mirror arrangement of the heart is found, the severity of the manifestations will depend on the severity of the damage to the internal organs.
Complications
In the absence of concomitant diseases, dextrocardia does not pose any health hazard and does not affect life expectancy. However, the unusual location of nearby organs can make it difficult to diagnose other diseases and provoke such consequences as:

Diagnosis of dextrocardia
With a congenital form of pathology, it can be detected immediately after the birth of the child. The key task of diagnostics is to identify the localization of other organs and identify abnormal processes in them. In addition, other pathologies of the heart and blood vessels should be excluded.
The key diagnostic method is electrocardiography (ECG). For infants, the procedure is carried out after the use of sedatives. Otherwise, there is a risk of disrupting the recording of the electrocardiogram and obtaining incorrect information.
If an ECG is performed with dextrocardia with the usual application of electrodes, with a mirror arrangement of the heart, teeth of the opposite direction can be detected. It should be borne in mind that dextrocardia on the ECG has an important feature: it is characterized by a sharp drop in voltage. 
It is necessary to take an ECG to diagnose other cardiac pathologies by applying a yellow electrode to the right hand. In this case, red - should be placed on the left hand.
The examination scheme necessarily includes ultrasound and x-rays. The first procedure is performed to examine the abdominal organs.
Radiography makes it possible to identify the pathological location of the heart. If a person has dextrocardia, an x-ray and description will give a clear picture of the heart and its contours. Such a snapshot helps to detect all changes.
In addition, the following studies can be carried out:

Important: The most significant diagnostic method is electrocardiography. It is this procedure that allows you to confirm or refute the diagnosis. It also allows you to choose methods for differential diagnosis.
Treatment
In most cases, dextrocardia is asymptomatic, so treatment is not carried out. If the baby has heart problems, it may be necessary to perform an operation. If necessary, before surgery, the child is prescribed drugs that increase the intensity of the heartbeat and reduce pressure.
If a person has Kartagener's syndrome, he is prescribed symptomatic remedies:
- expectorants and preparations for cleansing mucus;
- diuretics;
- to reduce pressure;
- antibiotics to eliminate bacterial complications.
 Typically, people with this diagnosis do not experience a decrease in life expectancy. With an isolated form of anomaly, congenital malformations are much more common, which increases the likelihood of dangerous health consequences.
Typically, people with this diagnosis do not experience a decrease in life expectancy. With an isolated form of anomaly, congenital malformations are much more common, which increases the likelihood of dangerous health consequences.
Many people are interested in whether they take the army with such a diagnosis. With the normal functioning of the internal organs, this condition is not a basis for exemption from military service. In the presence of abnormal changes, the decision on the suitability of the conscript is made by a special commission.
Prevention
Since the disease is congenital in nature, it can be very problematic to find effective prevention. At the stage of pregnancy planning, you should consult with a geneticist. This will help select adequate therapy to prevent dextrocardia in the fetus.
Sick children are prescribed medications and supportive care for preventive purposes. This will help prevent the progression of the disease. Usually such people are forced to take medicines and dose physical activity all their lives.
Dextrocardia is a pathology that only in certain cases can lead to various complications. But in order to avoid negative consequences for health, it is necessary to consult a doctor in a timely manner and strictly follow his recommendations.
Do you have any questions? Ask them in the comments! They will be answered by a cardiologist.
Peculiar ECG changes are observed in individuals with dextrocardia. They are characterized by the opposite direction of the main teeth compared to the usual direction.
So, in lead I, negative P and T waves are detected, the main tooth of the QRS complex is negative, and a QS complex is often recorded. There may be deep Q waves in the chest leads, which may give rise to an erroneous diagnosis of macrofocal changes in the myocardium of the left ventricle.
The figure shows an ECG of a healthy 40-year-old man with dextrocardia. When registering an ECG with the usual arrangement of electrodes, ventricular complexes of the QS type, negative T and P waves in leads I and aVL, and a deep Q wave in V 5 are noted.
When registering an ECG with the opposite overlay of red and yellow electrodes and right chest leads, these changes disappear. Only splitting of the QRS complex in leads III and aVF is noted, indicating a focal impairment of intraventricular conduction.
"Practical electrocardiography", V.L. Doshchitsin

In some cases, variants of a normal ECG associated with a different position of the axis of the heart are mistakenly interpreted as a manifestation of a particular pathology. In this regard, we will first of all consider the "positional" variants of the normal ECG. As mentioned above, healthy people may have a normal, horizontal or vertical position of the electrical axis of the heart, which depends on the physique, age and ...

A normal ECG with a horizontal position of the electrical axis of the heart must be distinguished from signs of left ventricular hypertrophy. In the vertical position of the electrical axis of the heart, the R wave has a maximum amplitude in leads aVF, II and III, in leads aVL and I a pronounced S wave is recorded, which is also possible in the left chest leads. ÂQRS = + 70° - +90°. Such…
When the heart rotates around the longitudinal axis clockwise (when viewed from the apex), the right ventricle goes forward and up, and the left ventricle goes back and down. This position is a variant of the vertical position of the axis of the heart. At the same time, a deep Q wave appears on the ECG in lead III, and occasionally in lead aVF, which can simulate signs of ...

Dextrocardia (from the Greek καρδία - heart and Latin dexter - right) is a developmental anomaly in which the heart occupies a “right-sided” position in the chest (normally, the heart is located mostly in the left half of the chest). The location of the great vessels may correspond to the chambers of the heart, but in some cases dextrocardia is combined with transposition of the great vessels.
For the first time, the abnormal right-sided location of the heart in the chest was described by the surgeon and anatomist from Italy, Hieronymus Fabricius (in 1606). The term dextrocardia appeared a little later (in 1643) thanks to his compatriot and colleague Marco Aurelio Severino.
At the moment, hereditary (autosomal recessive type of inheritance) and genetic (gene mutations in the first trimester of pregnancy) factors for the development of anomalies have been scientifically proven.
The defect is quite rare, it occupies 1.5-5% of all congenital heart defects, on average 1:8000-1:25000 newborns.
Distinguish:
- isolated dextrocardia (only the heart is incorrectly located; synonyms: right-handed right heart - about 39%);
- dextrocardia as part of situs viscerus inversus (mirror arrangement of all or some unpaired internal organs; synonyms: mirror dextrocardia, left-handed right heart - approximately 34%).
Dextrocardia can be combined with transposition of the great vessels of the D or L type.
Dextrocardia is often combined with other congenital malformations of the heart (VSD, ASD, tetralogy of Fallot ...) or other organ systems (Kartagener's syndrome - dextrocardia + bronchiectasis + sinusitis).
Clinical manifestations
If the structure of the main vessels in relation to the chambers of the heart is not changed and the direction of blood flow is generally not disturbed, then dextrocardia usually does not manifest itself. The anomaly is detected incidentally when taking an ECG or chest X-ray.
If dextrocardia is accompanied by other heart defects, then children often experience a lag in physical development and weight gain, more frequent diseases of the respiratory system, a more protracted course infectious diseases. The skin is often pale, with the development of severe heart failure, cyanosis may be observed.
Approximately 25% of patients with dextrocardia have a combined defect of the cardiovascular and respiratory systems - Kartagener's syndrome. It is manifested by frequent sinusitis, otitis, chronic bronchitis, frequent pneumonia. Men are often diagnosed with infertility.
If dextrocardia is part of situs viscerus ambiguous (literally - "uncertain position of the organs"), then symptoms of damage to other internal organs may appear. In asplenia, infections often develop and recur.
If there are combined heart defects, then the clinic is due to a variety of circulatory disorders (“cyanotic crises” with Fallot's tetrad, hypertrophy of the heart chambers and possible pulmonary hypertension with septal defects, etc.).
Abnormalities detected on physical examination
- The apex beat is palpated in the right intercostal space somewhat to the right of the right midclavicular line (normally at the same level on the left). In the region of the apex, the heart is located as close as possible to the surface of the body, so here its contractions can be felt under the fingers.
- In the region of the apex beat (see above), the first heart sound is heard (normally, in the 5th intercostal space along the midline on the left).
- With isolated dextrocardia, percussion and palpation of the abdominal cavity reveals the normal location of the remaining internal organs.
With situs viscerus inversus, an abnormal arrangement of many internal organs is revealed (the left lung has 3 lobes, and the right one has 2; the liver and gallbladder located on the left, the spleen may occupy a median position or be absent - asplenia).

An electrocarliogram with isolated dextrocardia has the following features:
- negative P wave in lead aVR;
- in lead aVL and left chest leads (V1-V6), a low voltage of the ECG teeth is determined;
- the R wave is largest in leads V1-V2 and smallest in V6 (normally it increases from V1 to V3, maximum in V4, and slightly decreases in V5-V6);
- in standard leads from the limbs I, II, III, the ventricular QRS complex looks like a QR;
- the transition zone of the chest leads (leads, where the R and S waves are approximately the same, normally - V3) is shifted to the right (V2).
In the case of mirror dextrocardia, the following are recorded on the ECG:
- negative P wave in leads I, aVL, V1-V6;
- the T wave in lead I is negative;
- in lead I, the main wave of the ventricular complex is directed downward from the isoline;
- decrease in R wave voltage in chest leads from V1 to V6;
- redistribution of leads aVL - aVR (they "swap places")
ECG removal with dextrocardia should be carried out "mirror" with the normal location of the chest electrodes. Then they are marked V1R-V6R.
Rg- diagnostics
With isolated dextrocardia, the apex of the heart is visualized in the right half of the chest, the rest of the organs are in their usual place.
With situs viscerus inversus - an abnormal location of the heart and other organs.
An inexpensive, harmless and very informative diagnostic method is echocardiography, which allows you to visualize the chambers of the heart online. Doppler echocardiography allows you to determine the direction of blood flow in the main vessels and chambers of the heart.
Fetal dextrocardia is diagnosed by fetal echoscopy.
Also, the location of the heart in the chest can be assessed using MRI or coronary angiography (usually performed for other heart defects and are not the main diagnostic methods).
Treatment and prognosis
 Dextrocardia - treatment and prognosis
Dextrocardia - treatment and prognosis If, with dextrocardia of the heart, the normal direction of blood flow in the vessels and chambers of the heart is preserved, then the anomaly (in this case there is usually no clinic) does not require treatment. The quality of life of these patients does not suffer.
People with isolated dextrocardia live normal lives. Children are born healthy, although heredity in the development of anomalies is noted.
However, very often dextrocardia is combined with other heart defects that can cause heart failure. In this case, it is necessary to correct the concomitant defect. Usually this is a surgical intervention, in some cases it is possible to use minimally invasive technologies.
Treatment of concomitant pathology of other organ systems, respectively, is the same as in the normal position of the heart.
6593 0
Dextrocardia
With dextrocardia (situs inversus), all parameters of the electrical position of the heart are mirrored to the right of the midline. The P wave will be inverted in lead I and the QRS axis (âQRS) will be tilted into the right lower quadrant (+90° to +180°). There will be no normal development of the complex from rS to qR to leads V5-V6 in the precordial leads, but it will be observed in leads located symmetrically on the right side of the chest (V3R-V6R) (Fig. 1). More often than dextrocardia, there is a situation in which electrodes incorrectly applied to the upper limbs simulate dextrocardia in the frontal plane, but this is not confirmed in the precordial leads.
Rice. 1. Dextrocardia. Note: mirror electrocardiographic patterns, all vectors are directed to the right. The right precordial leads register LV vectors, which are normally recorded on the left.
Repolarization
At the end of the QRS complex, the ECG returns to the baseline, where it remains for 150-200 ms before the onset of the T wave with its gentle onset and steep return to the baseline. The period between the end of the QRS complex and the beginning of the T wave is called the ST segment, and the connection of the QRS complex and the ST segment is called the J point. The ST segment can be slightly elevated above the isoline (0.5-1 mm) in leads with a high R wave, as well as in right precordial leads (V1-V2) with a dominant S wave. The most common variant of the norm, manifested by ST elevation ≥1 mm in many leads, is called the "early repolarization" syndrome. Often it is due to an increase in the tone of the vagus nerve and may serve as a reason for differential diagnosis with pericarditis or myocardial ischemia (Fig. 2).

Rice. 2. "Early repolarization" syndrome in a healthy 20-year-old man. Note ST-segment elevation in most leads, stable over time, without any symptoms of heart disease. Note also the high QRS voltage in the inferior and precordial leads, which could indicate LV enlargement, but this is normal for a 20 year old. The blue arrow points to a normal low-amplitude U wave.
The T wave is normally positive in leads I, II, aVL, and V2-V6, but may be different in other leads. The mean axis of the T wave (âT) in the leads in the frontal plane is ‹60° with respect to the âQRS. The T wave may be negative in the right precordial leads (V1-V3) in children until there is no loss of RV physiological dominance, and is also normal in Black African women and men.






